HRYA
Human Rights Youth Advocacy
Analysis, Literature Review
Published date:
December 25, 2023
|
Health Disparities in Asthma
Emma Ma
1. Introduction
Asthma is a heterogeneous disease characterized by inflammation in the respiratory airways and has a long history dating back to 2600 B.C. in China, but it cannot be cured completely. Approximately more than 27 million people have suffered from asthma, which is equivalent to 1 in 12 people. Among them, Black and Indigenous American adults show the highest rate of getting asthma in the U.S. The prevalence of childhood asthma among Puerto Ricans (19.2%) or non-Hispanic blacks (12.7%) is higher than among non-Hispanic whites (8%) or Mexican Americans (6.4%). Similarly, individuals from lower socioeconomic status (SES) often face challenges accessing healthcare, affording medications, and maintaining asthma control compared with those of high SES. The financial cost of asthma exceeds $81 billion every year. Despite substantial investments in resources, the disease leads to more than 3,500 deaths each year in the country. It commonly presents with variable symptoms of wheezing, shortness of breath, chest tightness, and cough. However, the combination of symptoms and airflow limitation can vary in frequency and intensity, which is typically caused by airborne allergens, such as pollen, dust mites, pet dander, or particles of cockroach waste among other factors. While significant health disparities exist, this research paper aims to explore important factors that trigger asthma and health disparities in it, focusing on the socioeconomic and racial/ethnic factors that contribute to differential outcomes in asthma prevalence, management, and overall health. This paper will also highlight recent trends that manifested the growth of asthma in the past few years.
2. Recent Trends
Reports have shown that Black-identifying individuals are more prone to suffer from asthma than others, as shown in Figure 1. The Centers for Disease Control and Prevention report conducted a bar graph to represent uncontrolled asthma among children from 2012 to 2014. Among these children from ages 0 to 17, females and babies show a higher prevalence of asthma (Figure 2). However, a recent study has shown changes between different racial, age and gender groups; males show a significant increase in asthma, but Black-identifying individuals have decreased in effectiveness, and children aged 0 to 11 are generally equally affected by the disease (Figure 3). Boys are more likely to develop childhood asthma than girls, at least until puberty. This disparity is attributed to the smaller size of airways in boys compared to girls under 10, leading to increased airway reactivity compared to girls of the same age, height, and weight. While boys have a higher risk of developing asthma, the trend may shift after puberty, with adult females being more vulnerable compared to adult males in adolescence and adulthood (Figure 4). Female lungs are often smaller and airways narrower than in males of similar age and size; they have more exposure to dust mites, molds, pets in the home or certain occupations like cleaning.
Furthermore, researchers have suggested that the clinical presentation of asthma may differ between males and females. For instance, females may experience more frequent and severe symptoms, along with comorbid conditions such as anxiety and depression. Therefore, investigating these gender-specific aspects of asthma symptomatology is vital for tailoring effective treatment approaches.
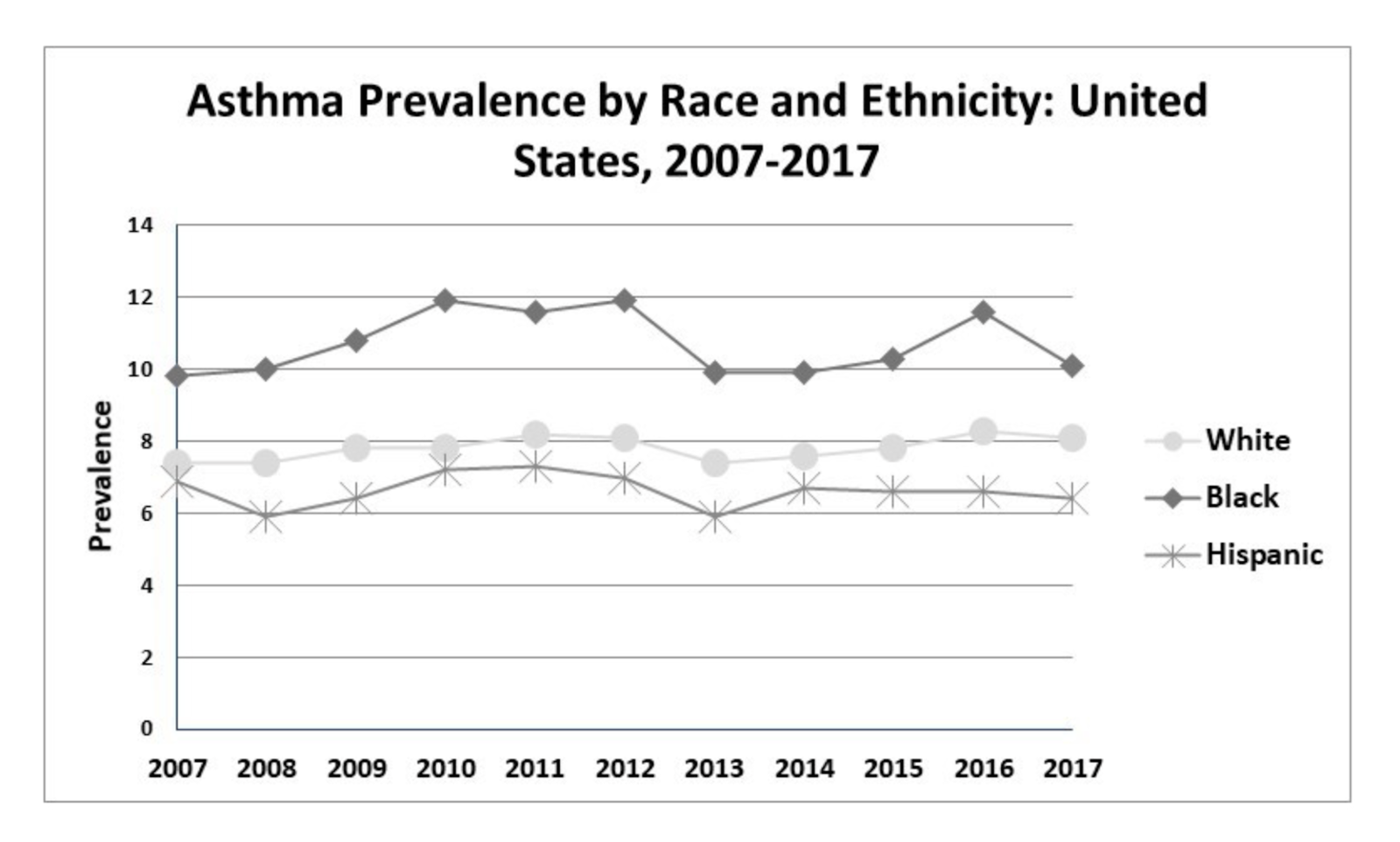
Figure 1: Trend in asthma prevalence in the US among Whites, African Americans and Hispanics from 2007 to 2017.
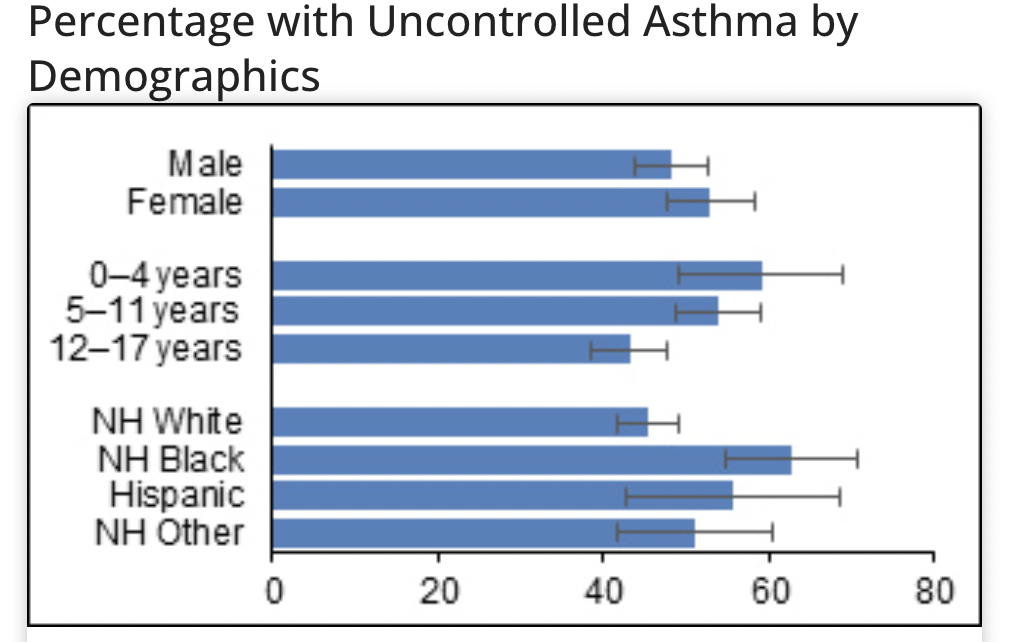
Figure 2: Percentage of uncontrolled asthma for children from 2012 - 2014.
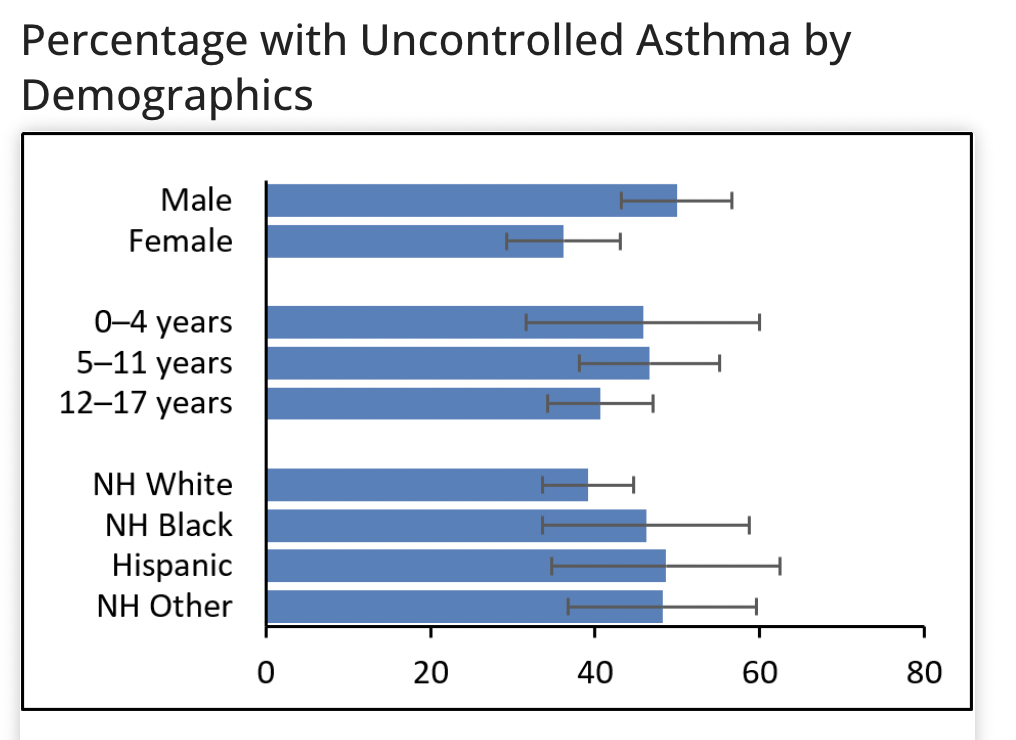
Figure 3: Percentage of uncontrolled asthma for children from 2018 - 2020.
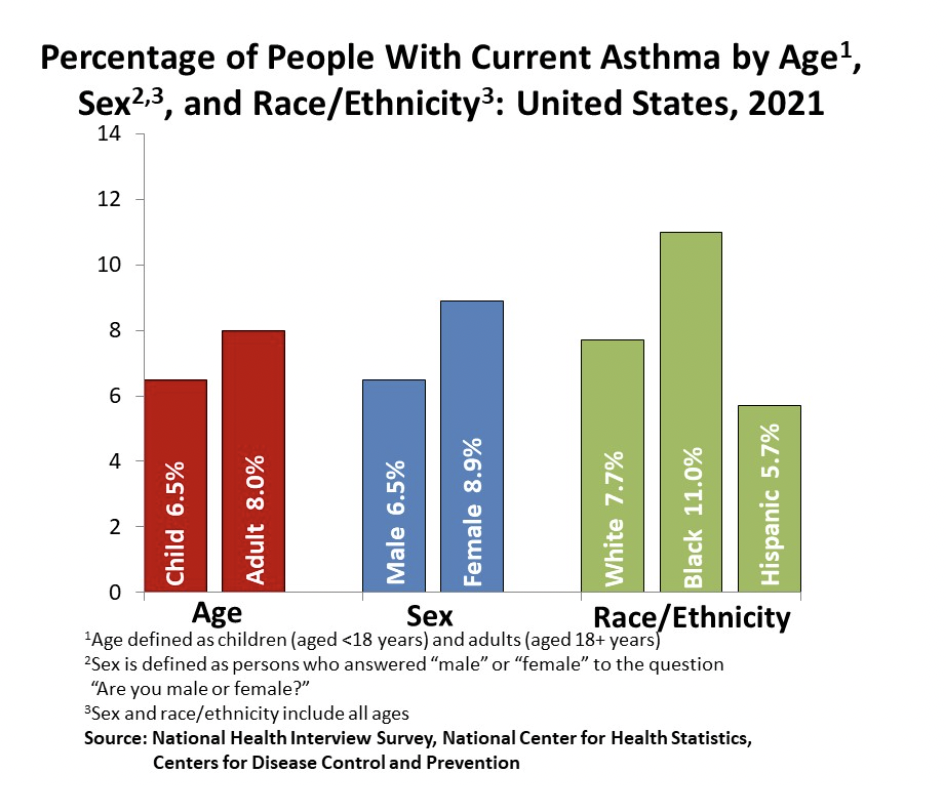
Figure 4: Percentage of people with current asthma by age, sex, and race/ethnicity in the U.S. 2021.
3. Causes and Effects
While the exact cause of asthma remains unidentified, various factors are known to influence the occurrence of asthma. Genetic factors, including a family history of asthma, play a significant role in increasing the risk of developing the condition. Studies suggest that over 100 genes may be associated with allergic asthma, although each appears to impact specific populations. Additionally, environmental exposures contribute to asthma development, with allergens such as pollen, dust mites, mold, pet dander, irritants like tobacco smoke, air pollution, and occupational exposures all playing roles. Furthermore, severe respiratory infections, particularly during early childhood, have been recognized as another factor that can elevate the risk of developing asthma. Besides these common triggers, socioeconomic and racial disparities can result in a higher chance of being exposed to asthma. Individuals with lower affordability may face higher rates of asthma prevalence due to limited access to healthcare, substandard living conditions, occupational health protections, and increased exposure to environmental triggers. Another consequence of the inferior social status is the lack of education; with limited health literacy, individuals may struggle to understand and follow asthma treatment instructions, leading to suboptimal control of the condition. Similarly, racial and ethnic minority groups may encounter barriers such as lack of insurance, limited access to primary care, and systemic biases in healthcare, leading to delayed or inadequate asthma management.
Although the specific triggers can vary from person to person, everyone with asthma will be affected by the same dietary triggers including sulphites, preservatives, histamine-rich Foods, and dairy products. In addition, one must control their emotions effectively to avoid worsening the disease. Once asthma is triggered, it can cause airway inflammation in the body, narrowing the airways and making breathing difficult. Over time, chronic inflammation causes lung function to be reduced, impacting an individual's ability to engage in physical activities such as running, swimming, wrestling, soccer, and tennis. If not managed properly, asthma can eventually lead to long-term disability.
4. Diagnosis & treatment
As mentioned previously, asthma is a condition characterized by the narrowing and swelling of an individual’s airways, leading to symptoms such as wheezing, coughing, and episodic periods of chest tightness. To diagnose asthma, doctors will examine the patient’s medical history and associated personal habits to help understand the symptoms and causes. A physical exam will also be placed to look for signs of asthma or other related conditions; doctors will check the ears, eyes, nose, throat, skin and listen to your chest and lungs. If anything appears peculiar or unsure to the doctor, they may refer the patient to a specialist and take tests accordingly. The commonly used tests of small airway function are discussed below in Table 1. Although there is currently no cure for asthma, patients can choose between several types of treatments to help them live a normal and active life. Relieve inhalers can help relieve symptoms when they occur, and preventer inhalers can stop symptoms from developing. People can use combination inhalers to do both functions. In addition to inhalers, doctors may also suggest taking tablets if using an inhaler alone is not helping. Leukotriene receptor antagonists (LTRAs) and theophylline are the primary tablets to fight against asthma but include side effects such as headaches or tummy aches.
Furthermore, injections of medicines called biologic therapies may be recommended for certain people as they are not suitable for everyone. When asthma becomes more severe, surgeries called bronchial thermoplasty can be performed. This surgery works by passing a thin, flexible tube down your throat and into your lungs. Then, heat on the muscles around the airways to help stop them from narrowing and causing asthma symptoms. Nevertheless, there is no complete cure for this disease. The essential step for governments would be to implement and enforce policies increasing access to healthcare for children and adults with asthma, regardless of their ethnicity.
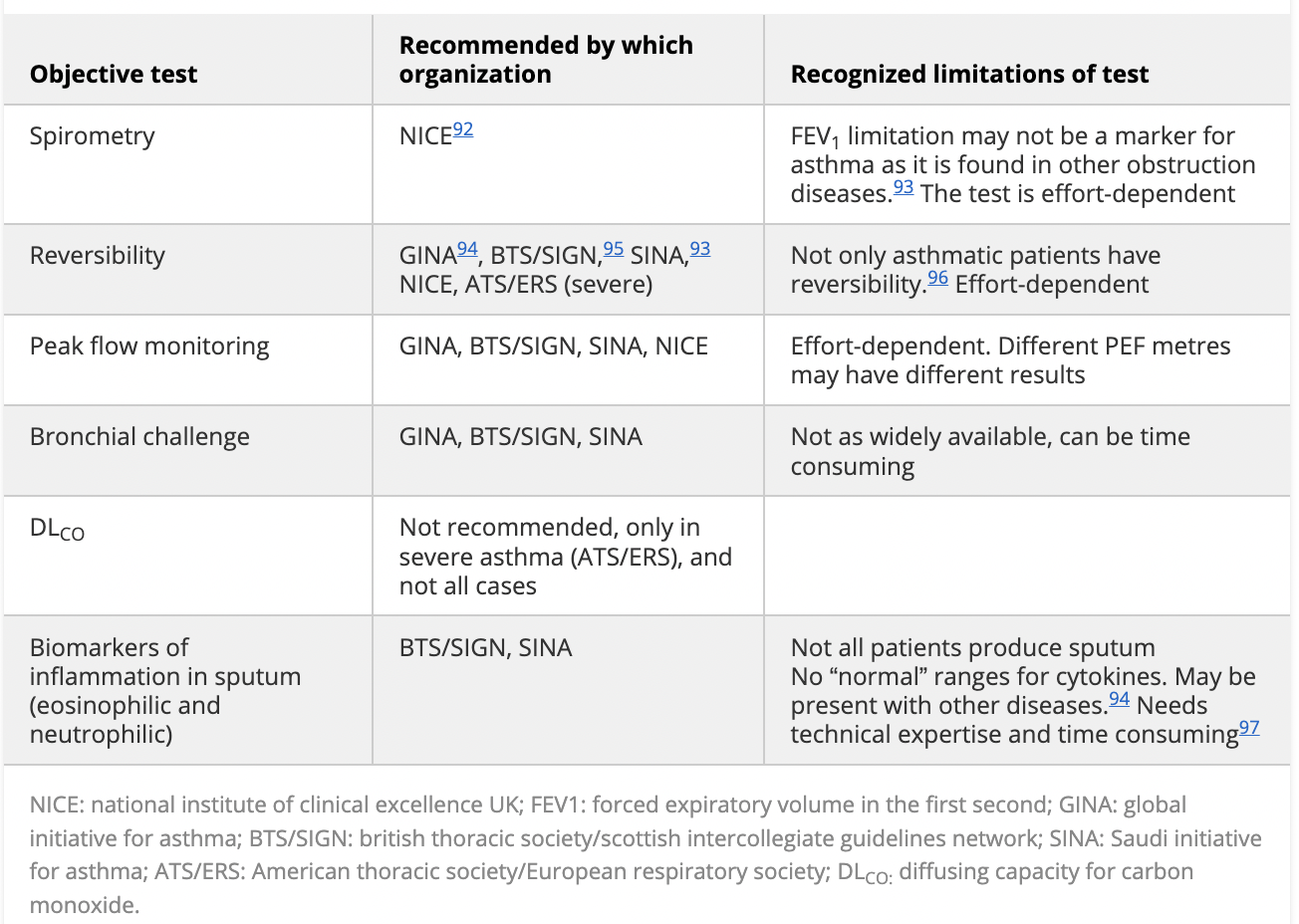
Table 1: Summary of objective tests used in diagnosing asthma by various organizations.
5. New Findings
Conducted by a professor at King’s College London, the SHAMAL study proposes that "severe asthma can be controlled using biologic therapies, without the addition of regular high-dose inhaled steroids which can have significant side effects." The study, spanning 22 sites across the UK, France, Italy, and Germany, revealed that 92% of patients treated with the biological therapy bevacizumab were able to safely reduce their intake of inhaled steroids, with over 60% of them successfully discontinuing the use of these steroids. The 208 patients were randomly assigned to decrease the dosage of high-dose inhaled steroids at various levels over 32 weeks, followed by a 16-week maintenance phase. Throughout the 48-week study duration, approximately 90% of the patients experienced no deterioration in asthma symptoms or exacerbations. Ultimately, the SHAMAL study suggests an alternative approach for controlling severe asthma by using biological therapies, such as bevacizumab. Although the new finding uncovers avenues for curing asthma, further research and clinical trials are needed to validate and refine these findings before the widespread implementation of treatment occurs.
6. Conclusions
The status of asthma involves ongoing research and advancements, with a focus on personalized treatment approaches, including biological therapies, to manage the condition better and minimize the use of high-dose inhaled steroids and their associated side effects. Despite novel discoveries for asthma treatment from the SHAMAL study, the primary barrier for potential or current asthma patients is the health and socioeconomic disparities that cause them a lack of education and affordability. As a result, all government agencies and policymakers must make transformative changes to equalize access to healthcare.
References
Asthma and Allergy Foundation of America. “Health Disparities.” Asthma & Allergy Foundation of America, 8 Nov. 2023, from https://aafa.org/advocacy/key-issues/health-disparities/
Centers for Disease Control and Prevention. (2019). AsthmaStats: Uncontrolled Asthma among Children, 2012–2014. U.S. Department of Health and Human Services. https://www.cdc.gov/asthma/asthma_stats/uncontrolled-asthma-children.htm
Forno, Erick. “American Journal of Respiratory and Critical Care Medicine.” ATS Journals, 2012, www.atsjournals.org/doi/full/10.1164/rccm.201202-0350ED.
Allergy & Asthma Network.“Asthma Disparities and Health Inequities=.” Allergy & Asthma Network, 2 Oct. 2023, https://allergyasthmanetwork.org/health-disparities/.
Trivedi, Michelle, and Eve Denton. “Asthma in Children and Adults-What Are the Differences and What Can They Tell Us about Asthma?” Frontiers in Pediatrics, U.S. National Library of Medicine, 25 June 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC6603154/#:~:text=Boys%20are%20more%20likely%20to,height%20and%20weight%20(21).
Almeshari, Mohammed A. “The Diagnosis of Asthma. Can Physiological Tests of Small Airways Function Help?” SageJournals, 2021, https://journals.sagepub.com/doi/full/10.1177/14799731211053332
King’s College London. “Major Breakthrough for Severe Asthma Treatment.” ScienceDaily, ScienceDaily, 8 Dec. 2023, www.sciencedaily.com/releases/2023/12/231208133135.htm.